
Acute coronary syndrome questions appear in 10–12 FRCEM SBA questions, with STEMI versus NSTEMI distinction being the most commonly tested pattern. Get this wrong and you're losing easy marks.
This guide explains the key differences between STEMI and NSTEMI, focusing on ECG interpretation and clinical decision-making that FRCEM actually tests.
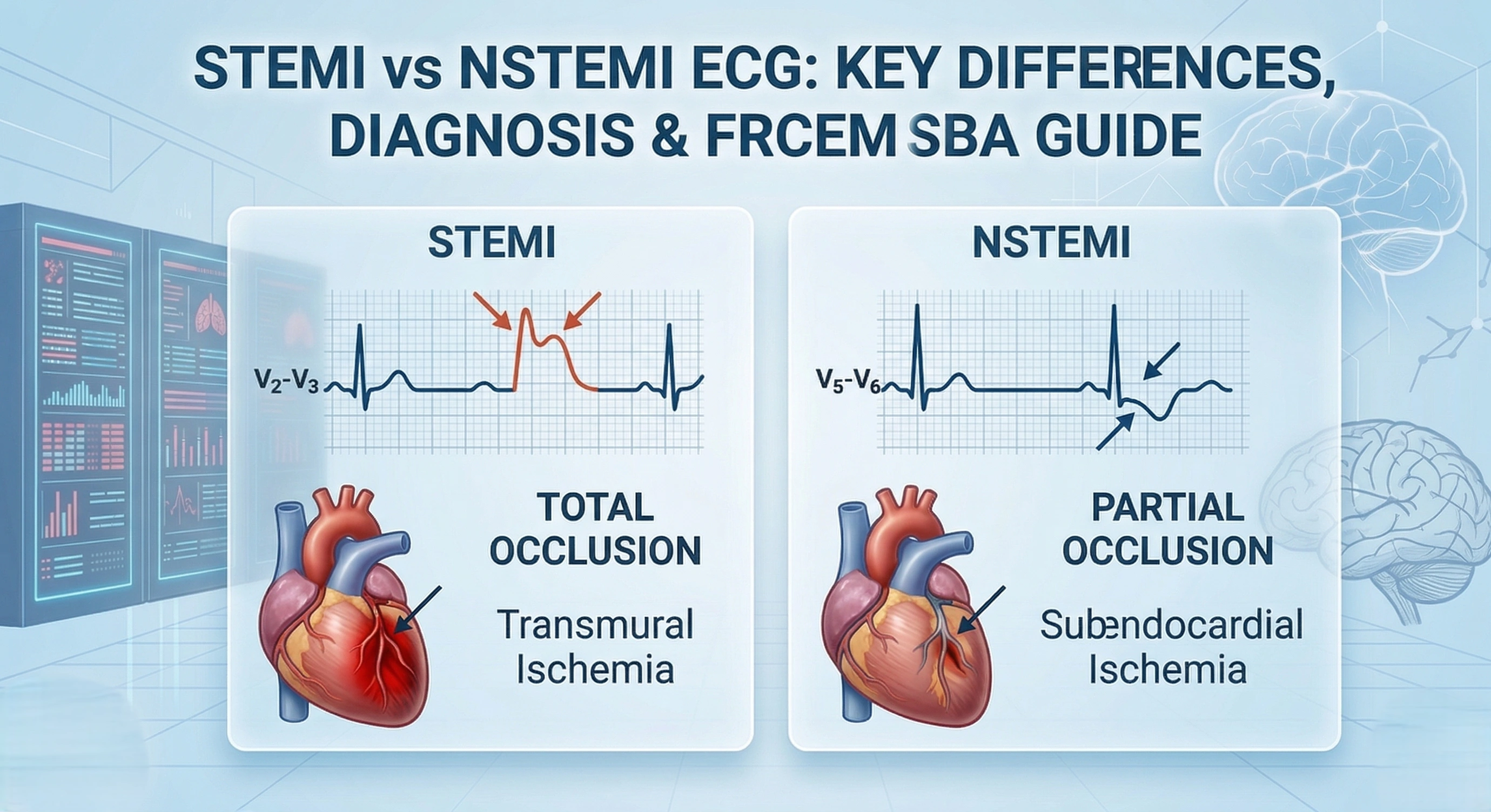
The Fundamental Difference
ST-Elevation Myocardial Infarction (STEMI):
Complete coronary artery occlusion
Transmural (full-thickness) myocardial infarction
ST elevation on ECG
Requires immediate reperfusion (cath lab or thrombolysis)
Time-critical emergency
Non-ST-Elevation Myocardial Infarction (NSTEMI):
Partial coronary artery occlusion
Subendocardial (partial-thickness) infarction
No ST elevation
Requires urgent but not immediate cath lab
Risk-stratified management
Key clinical distinction: STEMI = immediate cath lab activation. NSTEMI = urgent cardiology referral within 72 hours (sooner if high-risk).

STEMI ECG Criteria
Diagnostic ST elevation:
≥1mm (1 small square) in two contiguous limb leads, OR
≥2mm (2 small squares) in two contiguous chest leads
Territories:
Territory | Leads | Artery |
|---|---|---|
Anterior | V1–V4 | LAD |
Inferior | II, III, aVF | RCA |
Lateral | I, aVL, V5–V6 | Circumflex |
Posterior | Reciprocal depression V1–V3 + tall R waves | RCA/Circumflex |
Inferior STEMI tip: Always check right-sided leads (V3R, V4R) for RV involvement — avoid nitrates if RV infarct confirmed.
Posterior STEMI tip: Often missed on standard 12-lead. Get posterior leads V7–V9. Treat as STEMI.
NSTEMI ECG Patterns
Critical understanding: NSTEMI ECG can be completely normal (30% of cases).
Common NSTEMI ECG findings:
ST depression (horizontal or downsloping)
T wave inversion (deep, symmetrical)
Non-specific ST-T changes
Completely normal ECG
Most significant finding: Dynamic changes on serial ECGs (evolving ST depression or T wave inversion).
ST Depression in NSTEMI
Characteristics:
Horizontal or downsloping (not upsloping)
≥0.5mm (half small square)
Multiple leads (more significant than single lead)
FRCEM angle: Questions test understanding that ST depression indicates NSTEMI (or posterior STEMI if isolated to V1-V3), requiring urgent but not immediate intervention.

T Wave Changes in NSTEMI
Deep T wave inversion:
Symmetrical, deep (>2mm)
Biphasic T waves in some leads
Dynamic changes more significant than static findings
Wellens' syndrome (NSTEMI equivalent):
Deep symmetrical T wave inversion V2-V4
Indicates critical LAD stenosis
High risk of massive anterior MI
Requires urgent cardiology referral despite minimal troponin rise
FRCEM testing: Questions about Wellens' pattern test recognition of high-risk NSTEMI requiring urgent intervention despite non-dramatic ECG.
Key ECG Differences Summary
Feature | STEMI | NSTEMI |
|---|---|---|
ST elevation | Yes (≥1-2mm) | No |
ST depression | Reciprocal only | Primary finding |
T wave inversion | Develops later | Often present acutely |
Q waves | Develop over hours-days | Rarely develop |
Normal ECG | Never | 30% of cases |
Territoriality | Follows vascular distribution | May be widespread |
Dynamic changes | Evolves predictably | Most significant feature |
Troponin: The Diagnostic Separator
Both STEMI and NSTEMI have elevated troponin. ECG distinguishes them, not troponin level.
Troponin rise timing:
Detectable: 3-4 hours post-symptom onset
Peak: 12-24 hours
Elevated for: 7-14 days
High-sensitivity troponin:
Allows earlier detection
0-hour and 3-hour protocols common
FRCEM angle: Questions presenting chest pain with normal ECG and normal troponin at 2 hours—correct answer is repeat troponin at 3-6 hours, not discharge based on single troponin.
Management: Key Differences
STEMI
Aspirin 300 mg
Immediate cath lab — FMC-to-balloon target: 120 minutes
Add P2Y12 inhibitor: prasugrel preferred over ticagrelor for patients going to PCI
Prasugrel: 60 mg load, then 10 mg daily
Ticagrelor: 180 mg load, then 90 mg twice daily (alternative)
UFH anticoagulation
Analgesia: IV morphine for severe pain
Oxygen only if SpO₂ <90% — do not give routine oxygen
Do NOT pre-treat with prasugrel or ticagrelor before coronary anatomy is known when early invasive management is planned — Class III in the latest ESC guidelines.
If PPCI unavailable within 120 minutes → fibrinolysis within 12 hours of symptom onset, then transfer for angiography within 3–24 hours.
NSTEMI
Risk stratification determines timing:
Risk | Timing | Features |
|---|---|---|
Very high | Immediate (<2 hrs) | Haemodynamic instability, refractory chest pain, life-threatening arrhythmia |
High | <24 hours | Confirmed NSTEMI, GRACE >140, dynamic ECG changes |
Intermediate | <72 hours | GRACE 109–140, diabetes, renal impairment, recurrent ischaemia |
Updated: Routine invasive management within 24 hours for all high-risk NSTEMI is now a Class IIa recommendation (downgraded from Class I) — "should be considered" rather than mandated.
STEMI Equivalents — Treat as Immediate PPCI
Posterior MI: ST depression V1–V3 + tall R waves → confirm with V7–V9 → treat as STEMI.
De Winter's T waves: Upsloping ST depression in precordial leads + tall prominent T waves + subtle ST elevation aVR → acute LAD occlusion → treat as STEMI.
New LBBB + chest pain: Use Sgarbossa criteria to confirm MI. Score ≥3 = treat as STEMI.
Concordant ST elevation ≥1 mm (5 points — most specific)
Concordant ST depression ≥1 mm in V1–V3 (3 points)
Discordant ST elevation ≥5 mm (2 points)
Common FRCEM Mistakes
Mistake 1: Missing posterior MI — ST depression V1–V3 isn't always NSTEMI. Check for tall R waves and get posterior leads.
Mistake 2: Normal ECG = no ACS — 30% of NSTEMI have normal initial ECG. Always do serial ECGs and serial troponins.
Mistake 3: Confusing STEMI time targets — FMC-to-balloon is 120 minutes (PPCI vs fibrinolysis decision). Door-to-balloon 90 minutes is an in-hospital performance metric.
Mistake 4: Giving routine oxygen — only if SpO₂ <90%.
Mistake 5: Pre-treating with prasugrel/ticagrelor before anatomy known — not recommended in the latest guidelines.
Mistake 6: Missing Wellens' syndrome — biphasic or deeply inverted T waves V2–V4 with near-normal troponin is high-risk, not reassuring.
Frequently Asked Questions
Can STEMI have ST depression?
Yes, as reciprocal changes in leads opposite the infarct territory. But there's always primary ST elevation somewhere.
What if ECG shows both ST elevation and depression?
Identify the primary ST elevation (STEMI), treat accordingly. Depression is likely reciprocal.
How quickly do STEMI ECG changes evolve?
Hyperacute T waves appear within minutes, ST elevation within 30-60 minutes, Q waves develop over hours to days.
Do troponin levels differ between STEMI and NSTEMI?
Troponin elevation occurs in both. STEMI often has higher peak levels but overlap exists. ECG distinguishes them, not troponin level.
What about STEMI mimics?
Pericarditis, Brugada pattern, and early repolarization can show ST elevation. Distinguish by distribution, morphology, and clinical context.
STEMI versus NSTEMI distinction is fundamental to FRCEM cardiology questions. Master the ECG criteria (1mm limb, 2mm chest for STEMI), understand that NSTEMI can have normal ECG, and recognize STEMI equivalents requiring immediate intervention.
The key isn't memorizing rare variants—it's rapidly identifying STEMI requiring immediate cath lab versus NSTEMI requiring urgent but not immediate intervention. This time-critical decision-making is exactly what FRCEM tests.
Ready to master ACS recognition with comprehensive ECG practice? Register with StudyFRCEM for SLO-mapped cardiology questions including STEMI/NSTEMI scenarios with detailed ECG interpretation.
Guidelines referenced:
ESC Guidelines for the Management of Acute Coronary Syndromes (latest) — escardio.org
NICE NG185: Acute Coronary Syndromes (latest) — nice.org.uk