
Overdose presentations are some of the most time-pressured scenarios in emergency medicine — and some of the most reliably tested in the FRCEM SBA paper. Paracetamol and tricyclic antidepressant (TCA) overdose appear together in roughly 6–8 questions per sitting, and they test two completely different skill sets.
Paracetamol questions are largely about getting the decision points right: when to treat, what the nomogram threshold is, what happens with staggered ingestions. TCA questions are about recognising the ECG changes fast and knowing exactly what to do when a patient is deteriorating. Confuse the approaches, or misremember a number, and straightforward marks disappear.
This guide covers both conditions the way FRCEM actually tests them — with the clinical scenarios, exact numbers, and management steps that come up again and again. Work through this alongside your full FRCEM toxicology preparation and you'll have the right answers committed to memory before exam day.
Part 1: Paracetamol Overdose
Paracetamol is the most common drug overdose seen in UK emergency departments. It's also one of the most preventable causes of acute liver failure — which is exactly why FRCEM tests it in detail.
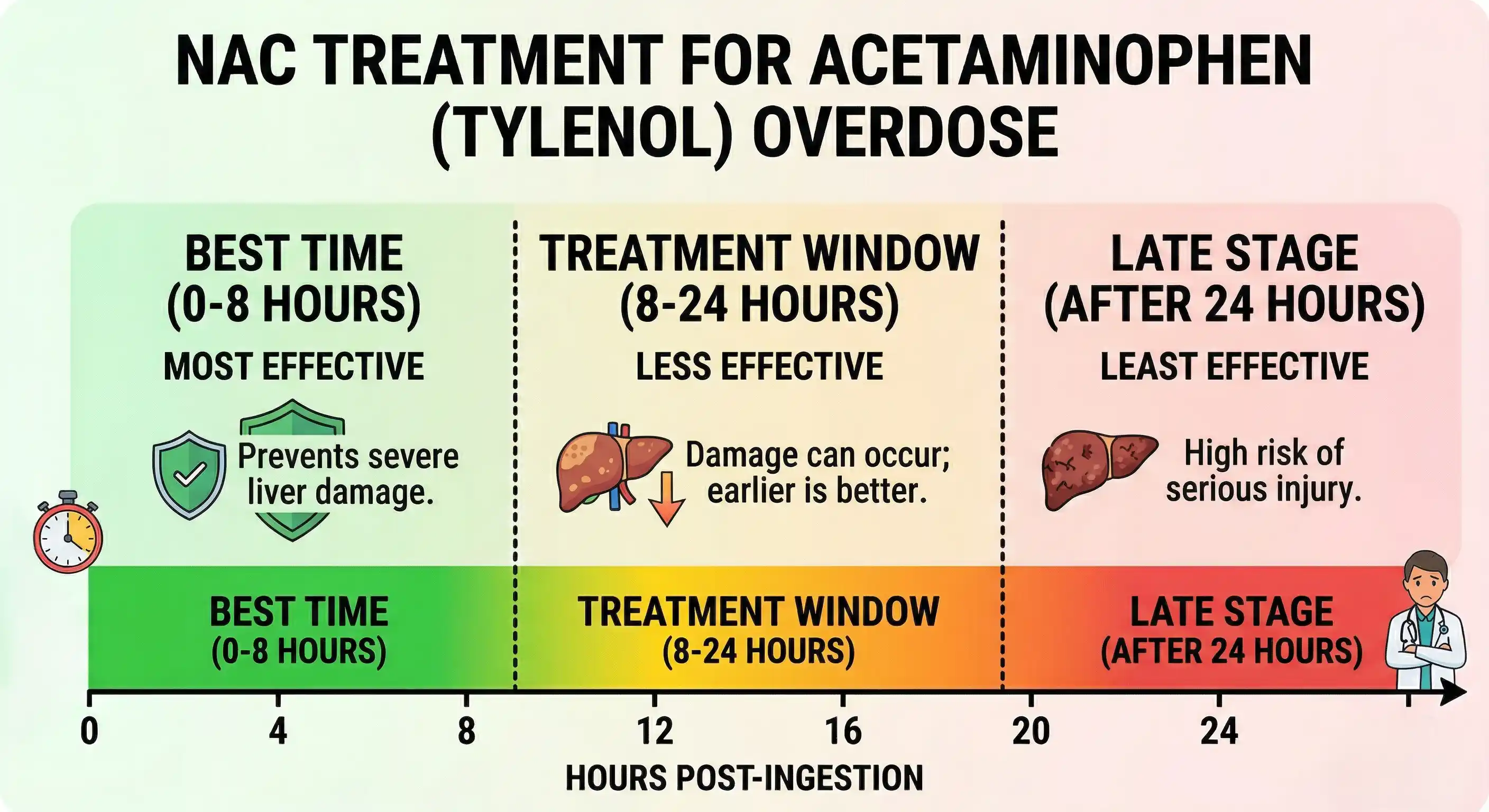
Why It Matters: The 8-Hour Window
This is the single most important concept in paracetamol overdose management.
NAC (N-acetylcysteine) — the antidote — has near 100% efficacy in preventing hepatotoxicity if given within 8 hours of ingestion. After 8 hours, efficacy falls substantially. After 24 hours, liver failure may already be established.
Every paracetamol question in FRCEM comes back to this: is the patient within the window, and does the level cross the treatment threshold?
The Nomogram: One Line, Not Two
If you've studied older resources, you may have seen two treatment lines on the paracetamol nomogram — one for "high-risk" patients (with risk factors like alcohol, malnutrition, enzyme inducers) and one standard line.
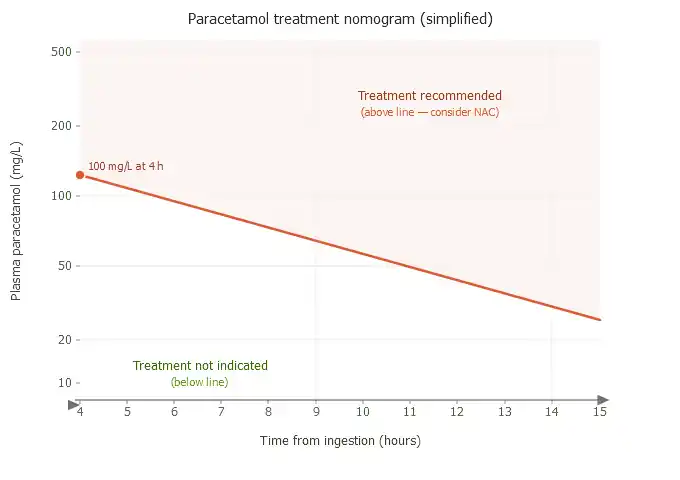
That two-line system is obsolete. The UK now uses a single treatment line at 100 mg/L at 4 hours.
Following a review by the Commission on Human Medicines (MHRA), risk factor assessment was abandoned because the evidence base was poor and inconsistent. The risk factors were difficult to assess accurately in a time-pressured ED setting, and patients died as a result of being incorrectly classified as "low risk."
The current single nomogram line:
Paracetamol level ≥100 mg/L at 4 hours = treat with NAC
A single treatment threshold applies to all patients, regardless of risk factors
The old "high-risk line" at 50 mg/L is no longer used in the UK. If a question refers to risk factor stratification using two nomogram lines, the current answer is that this system has been replaced.
When the Nomogram Cannot Be Used
This is tested frequently. The nomogram is only reliable for acute single ingestions where the timing is certain. In several important scenarios, it cannot be applied:
Staggered overdose (ingestion over more than 1 hour): Treat with NAC immediately — do not wait for a level or try to plot on the nomogram. The nomogram assumes a single acute ingestion; staggered ingestions produce unpredictable levels that don't correlate with the graph.
Unknown time of ingestion: Treat with NAC immediately. When in doubt, treat.
Time of ingestion >15 hours ago: The nomogram becomes unreliable after 15 hours. Seek NPIS (National Poisons Information Service) guidance — treatment decisions should be individualised based on clinical status and liver function tests.
Paracetamol level above or twice the nomogram line: Discuss with NPIS/toxicology. Patients with levels ≥300 mg/L require specialist input.
NAC Dosing: Standard Regime vs SNAP
Two regimens are in use across UK emergency departments:
Standard 3-bag regime (21 hours total):
Bag 1: 150 mg/kg in 200 ml glucose over 60 minutes
Bag 2: 50 mg/kg in 500 ml glucose over 4 hours
Bag 3: 100 mg/kg in 1 litre glucose over 16 hours
SNAP regime (Scottish and Newcastle Acetylcysteine Protocol — 12 hours total):
Infusion 1: 100 mg/kg over 2 hours
Infusion 2: 200 mg/kg over 10 hours
The SNAP regime is now recommended by RCEM and increasingly adopted across UK EDs. It delivers the same total NAC dose as the standard regime but over 12 hours instead of 21, with fewer adverse reactions and shorter length of stay. FRCEM awareness of both regimes is appropriate — know SNAP exists and that it's RCEM-endorsed.
Note on the first infusion: The initial NAC infusion is given over 60 minutes (not 15 minutes as in older protocols) — this significantly reduces the frequency of anaphylactoid reactions, which are directly related to peak serum NAC concentration.
Activated Charcoal
Consider if the patient presents within 1 hour of ingestion and has consumed more than 150 mg/kg. Ensure the airway is protected — do not give charcoal to a drowsy or combative patient.
When to Continue NAC Beyond the Planned Regime
NAC should be continued (at the rate of the third bag, 100 mg/kg over 16 hours) if at the end of treatment:
ALT has more than doubled from admission measurement
ALT is ≥2× the upper limit of normal
INR >1.3 (not explained by anticoagulant therapy)
Continue until INR ≤1.3 or is falling on two consecutive measurements and is <3.0.
Investigations in Paracetamol Overdose
At 4 hours post-ingestion (minimum):
Plasma paracetamol level (plot on nomogram)
LFTs, INR, U&E, creatinine, glucose, FBC
VBG
If NAC is started: Repeat LFTs, INR, creatinine at completion of each bag. More frequent monitoring if clinical deterioration.
Signs of established hepatotoxicity (which FRCEM may present as a worsening scenario):
Rising ALT/AST (can peak >10,000 IU/L in severe cases)
Coagulopathy (rising INR)
Hypoglycaemia
Encephalopathy
Renal impairment
Any patient with these features requires urgent liver team involvement and consideration for transfer to a liver transplant centre.
NAC Hypersensitivity Reactions
Anaphylactoid reactions occur in up to 15% of patients during NAC infusion — most commonly in the first bag. These are not true anaphylaxis and are not a contraindication to continuing treatment.
Management:
Slow or pause the infusion
Give antihistamine (chlorphenamine) and/or salbutamol if bronchospasm
Once reaction settles, restart at a slower rate
The benefit of NAC always outweighs the risk of not treating
FRCEM specifically tests whether hypersensitivity is a contraindication (it is not).
Safe Discharge Criteria
Not every patient who takes paracetamol needs NAC. Patients with a level below the nomogram line following an acute single ingestion at a known time can be considered for discharge — but all patients who have taken a paracetamol overdose in the context of self-harm must have a psychiatric review before discharge, regardless of clinical status.
Part 2: Tricyclic Antidepressant (TCA) Overdose
TCA overdose is one of the most dangerous drug overdoses encountered in the ED. It can go from apparently stable to cardiac arrest in minutes — and FRCEM tests whether you can recognise the warning signs and act on them before that happens.
Mechanism: Why TCA Overdose Is So Dangerous
TCAs exert their toxicity through three main mechanisms:
Sodium channel blockade → slows myocardial conduction → QRS widening, ventricular arrhythmias, hypotension
Potassium channel blockade → QTc prolongation
Anticholinergic effects → tachycardia, dilated pupils, dry flushed skin, urinary retention, reduced GCS
Alpha-1 blockade → vasodilatation → hypotension
The cardiac effects are the most dangerous and the most tested.
Common TCAs in overdose: amitriptyline (most frequently implicated in serious toxicity), dothiepin/dosulepin, imipramine, clomipramine, nortriptyline.
Clinical Presentation
The classic TCA toxidrome — and FRCEM will present this as a clinical scenario:
Anticholinergic features: tachycardia, dry flushed skin, dilated pupils, urinary retention, confusion
Reduced GCS — can deteriorate rapidly
Seizures — often early, can precipitate fatal acidosis
Hypotension — from sodium channel blockade and alpha-1 antagonism
ECG changes — the most important findings (see below)
Rule of thumb for FRCEM: Any patient presenting with altered consciousness, tachycardia, and an unknown overdose — get an ECG immediately. TCA toxicity must be actively excluded.
ECG Changes: The Core of TCA Testing
The ECG is the most important tool in TCA overdose management. Know these changes and what they predict.
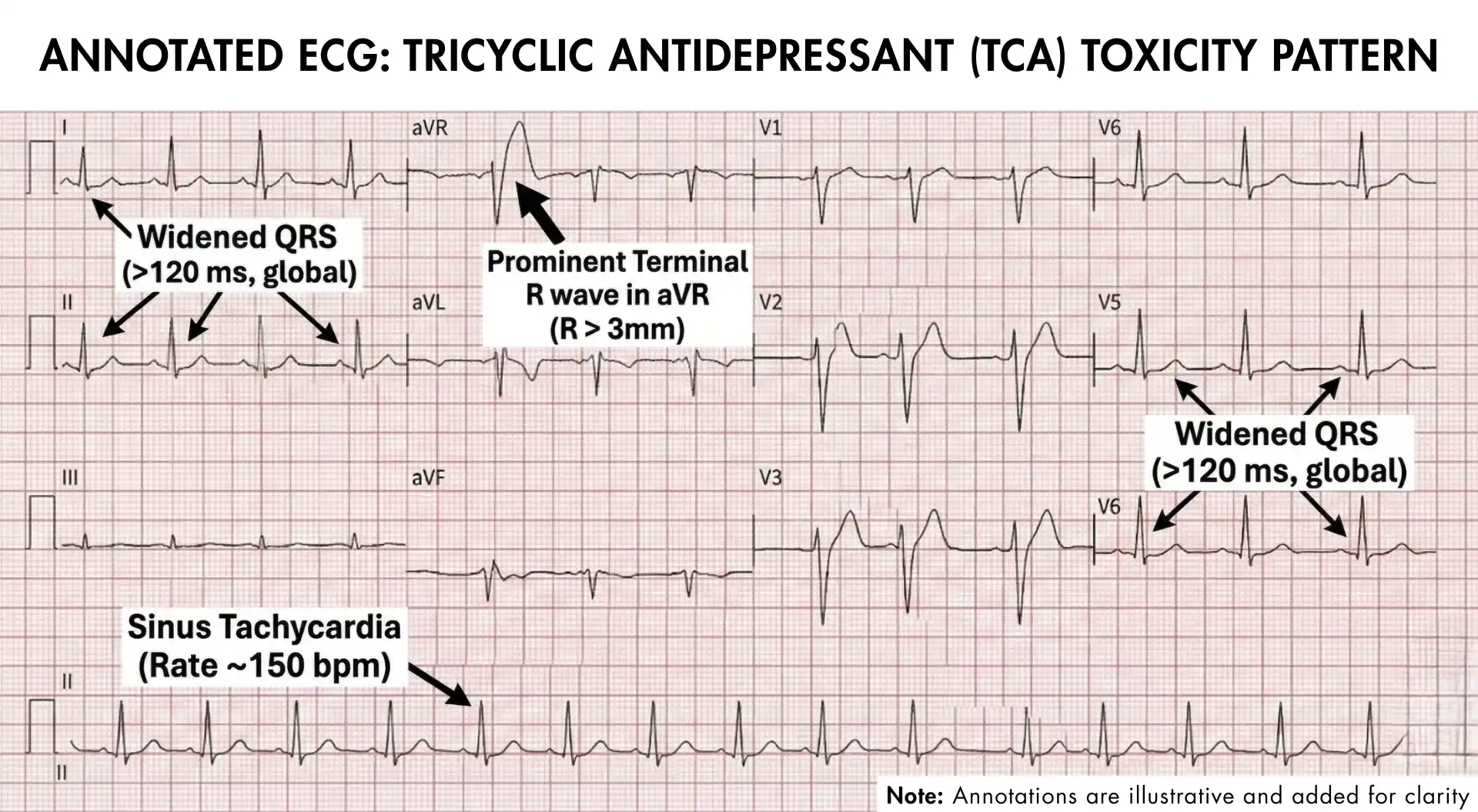
Key ECG findings in TCA overdose:
Finding | Significance |
|---|---|
Sinus tachycardia | Early and common — anticholinergic effect |
QRS widening (>100 ms) | Sodium channel blockade; predictor of seizures |
QRS >160 ms | High risk of ventricular arrhythmias (VT/VF) |
Dominant terminal R wave in aVR (>3 mm) | Highly specific for TCA toxicity |
R/S ratio >0.7 in aVR | Alternative marker of TCA toxicity |
QTc prolongation | Potassium channel blockade; risk of torsades |
The terminal R wave in aVR is the most FRCEM-specific finding — it results from terminal right axis deviation caused by preferential sodium channel blockade in the right intraventricular conduction system. When you see a tall positive deflection at the end of the QRS in aVR, think TCA.
ED Management: Step by Step
1. Immediate Stabilisation (All TCA Overdoses)
IV access, continuous cardiac monitoring, 12-lead ECG
High-flow oxygen
Baseline bloods: VBG (pH critical), U&E, glucose, paracetamol level (co-ingestion common)
2. Airway Management
TCA overdose carries a high aspiration risk due to rapid reduction in GCS. Adopt a low threshold for early intubation — don't wait for the patient to arrest before securing the airway.
Indications for RSI in TCA overdose:
GCS ≤12 (or rapidly deteriorating)
Inability to protect airway
Refractory seizures
Pre-cardiac arrest state
Use ketamine for induction — it's less proconvulsant and maintains blood pressure better than propofol in this context. Avoid succinylcholine if there is concern about hyperkalaemia from rhabdomyolysis; rocuronium with sugammadex available is preferable.
3. Sodium Bicarbonate — The Key Treatment
This is the most tested treatment decision in TCA overdose. Sodium bicarbonate works through two mechanisms:
Sodium loading — high serum sodium competes with TCA for cardiac sodium channels
Alkalinisation — alkaline pH (7.45–7.55) increases protein binding of TCA, reducing free drug levels
Give IV sodium bicarbonate when:
QRS >100 ms
Ventricular arrhythmias
Hypotension not responding to IV fluids
Seizures with ECG changes
Dose: 50–100 ml of 8.4% sodium bicarbonate (50–100 mmol) as IV bolus. Repeat as needed.
Target pH: 7.45–7.55. Do not exceed pH 7.55 — excessive alkalinisation risks paradoxical worsening of arrhythmias and hypokalaemia.
The key FRCEM principle: In TCA overdose, you give bicarbonate not primarily for acidosis, but to exploit the pH effect on sodium channel binding. A patient with a normal pH who has QRS widening should still receive bicarbonate.
4. Seizures
Seizures are particularly dangerous in TCA overdose because they cause acidosis, which increases free TCA levels, which worsens cardiac toxicity — a rapidly lethal cycle.
Benzodiazepines first (lorazepam or diazepam IV) — both treat seizures and provide some protection against TCA-induced seizures via GABAergic mechanisms
Avoid phenytoin — it has sodium channel blocking properties that can worsen TCA cardiac toxicity
If seizures continue despite benzodiazepines: intubate, propofol infusion, repeat benzodiazepines
5. Hypotension
Treat in order:
IV crystalloid bolus (0.9% saline or balanced crystalloid)
If refractory: sodium bicarbonate (may also improve hypotension from sodium channel blockade)
If still refractory: vasopressors — noradrenaline is preferred; avoid dopamine in TCA overdose
6. Activated Charcoal
Consider if the patient presents within 1 hour of ingestion AND the airway is protected (alert patient or already intubated). In most TCA overdoses presenting to the ED, the window has already passed or the patient's airway is at risk — exercise caution.
7. Drugs to Avoid in TCA Overdose
Drug | Why to avoid |
|---|---|
Phenytoin | Sodium channel blocker — worsens cardiac toxicity |
Flumazenil | If benzodiazepines co-ingested, reversal can precipitate seizures |
Class 1A/1C antiarrhythmics (e.g. flecainide, amiodarone) | Additional sodium channel blockade |
Physostigmine | Risk of asystole and seizures |
FRCEM specifically tests the flumazenil and phenytoin traps.
Monitoring and Disposition
ECG monitoring for all TCA overdose patients
Safe observation period: 6 hours from ingestion — patients who remain asymptomatic with a normal ECG, normal GCS, and no cardiovascular instability at 6 hours are at low risk of serious toxicity
Any ECG changes → ICU/HDU admission, regardless of apparent clinical stability
Patients who require bicarbonate, airway management, or vasopressors → ICU
Key Numbers for TCA Overdose
Threshold | Clinical significance |
|---|---|
>10 mg/kg ingested | Risk of coma, hypotension, seizures, arrhythmias |
>30 mg/kg | Severe toxicity with pH-dependent cardiotoxicity |
QRS >100 ms | Predictor of seizures — give bicarbonate |
QRS >160 ms | High risk of ventricular arrhythmias |
Target pH | 7.45–7.55 |
Safe observation | 6 hours from ingestion |
Paracetamol vs TCA: What FRCEM Tests Differently
Feature | Paracetamol OD | TCA OD |
|---|---|---|
Key danger | Hepatotoxicity (delayed 24–72 hrs) | Cardiac arrhythmia (within 6 hrs) |
Key investigation | Plasma paracetamol level + LFTs | ECG (QRS width, aVR) |
Main antidote | NAC (IV acetylcysteine) | Sodium bicarbonate |
Nomogram used? | Yes (single line, 100 mg/L at 4 hrs) | No |
Activated charcoal? | Within 1 hour if >150 mg/kg | Within 1 hour if airway safe |
Avoid | Delaying NAC beyond 8 hrs | Phenytoin, flumazenil |
Psychiatric review | All self-harm cases before discharge | All self-harm cases before discharge |
Key time window | 8 hours for NAC | 6 hours observation period |
Common FRCEM Mistakes
Mistake 1: Using two nomogram lines for paracetamol The single 100 mg/L line replaced the two-line system. Risk factor assessment is no longer performed. If a question presents a "high-risk" line at 50 mg/L as a current option, it's wrong.
Mistake 2: Using the nomogram for staggered overdose Staggered ingestion = give NAC immediately, no nomogram. This trips up many candidates who try to plot a level that was never designed to be plotted.
Mistake 3: Stopping NAC when LFTs are rising Worsening liver function at the end of the NAC regime is an indication to continue, not stop.
Mistake 4: Reassurance from a "normal" ECG early in TCA overdose ECG changes can evolve rapidly — a normal ECG at presentation doesn't mean the patient is safe. Six-hour observation is mandatory.
Mistake 5: Giving phenytoin for TCA seizures Benzodiazepines only. Phenytoin is contraindicated in TCA-associated seizures.
Mistake 6: Giving flumazenil to a TCA patient who co-ingested benzodiazepines This will precipitate seizures. Never give flumazenil if TCA overdose is suspected.
Mistake 7: Not treating QRS >100 ms with bicarbonate because pH is normal Bicarbonate is given for ECG changes regardless of baseline pH. The sodium loading and alkalinisation effects are beneficial even without established acidosis.
High-Yield FRCEM SBA Practice Cases
Theory is only half the battle. Can you spot the toxicology traps?
FRCEM examiners routinely hide critical details—like a staggered ingestion masquerading as a single dose, or a "normal" pH in a TCA patient who desperately needs Sodium Bicarbonate for QRS widening. Knowing the updated guidelines isn't enough; you have to apply them under pressure without falling for outdated nomogram distractors.
See exactly how Paracetamol and TCA cases look in the real exam.
👉 Take the Free FRCEM SBA Demo Now
Study Strategy
Toxicology questions in FRCEM reward systematic preparation more than almost any other topic. The management steps are protocol-driven, the numbers are specific, and the scenarios are predictable.
For paracetamol, prioritise:
The 8-hour window and NAC efficacy
Single nomogram line (100 mg/L at 4 hours)
Staggered overdose = treat immediately, no nomogram
When to continue NAC beyond the planned regime
Hypersensitivity reactions are not a contraindication
For TCA, prioritise:
ECG findings: QRS >100 ms, terminal R wave in aVR
Sodium bicarbonate: when, why, and pH target (7.45–7.55)
Drugs to avoid: phenytoin and flumazenil
6-hour observation rule
Low threshold for early intubation
Working through 40–50 toxicology SBA questions in the final preparation phase is recommended. For broader exam strategy, the FRCEM resuscitation and high-yield topics guide is worth pairing with this — the overlapping pharmacology (bicarbonate, seizure management) reinforces both areas.
Frequently Asked Questions
Do I need to know exact NAC doses for the exam?
Know the infusion sequence concept and that SNAP is the 12-hour RCEM-endorsed regime. You're unlikely to be asked for precise mg/kg numbers, but knowing the structure (two infusions for SNAP, three bags for standard) is useful.
Is SNAP the standard regime for FRCEM questions?
The standard 3-bag 21-hour regime remains referenced in most UK guidelines, but SNAP is increasingly used in practice and RCEM-endorsed. Know both exist; the clinical principles (same total dose, shorter time) are more important than memorising the specific infusion details.
What if a patient refuses psychiatric assessment after paracetamol OD?
Capacity assessment is required. If the patient has capacity and declines, document thoroughly. If capacity is impaired (e.g. by intoxication), consider treatment under the Mental Capacity Act. FRCEM may test the principle that psychiatric review is mandatory before discharge for self-harm.
How quickly can TCA toxicity develop?
Severe toxicity — including seizures and ventricular arrhythmias — typically manifests within 2 hours of ingestion. The greatest risk period for arrhythmias is within the first 6–8 hours. This is why the 6-hour observation rule exists.
Can you use the paracetamol level to guide treatment in severe overdose (level >300 mg/L)?
These patients require NPIS/toxicology input. Levels this high may indicate a risk of severe hepatotoxicity that warrants extended NAC treatment and close monitoring for fulminant liver failure.
Turn Toxicology Traps into Guaranteed Marks
Memorising the theory is only step one. To pass the FRCEM, you must apply these guidelines under time pressure against expert-level distractors.
Don't leave your score to chance. Register with StudyFRCEM to unlock our FRCEM SBA Question Bank and get instant access to:
Real Exam Simulation: High-yield, SLO-mapped toxicology cases.
Trap Navigation: Master staggered ingestions, flumazenil traps, and QRS widening.
Up-to-Date Explanations: Backed by the latest MHRA, RCEM, and NPIS guidelines.
👉 Start Practicing with StudyFRCEM Today
Guidelines referenced:
MHRA/CHM Paracetamol Overdose Guidance (single treatment line) — gov.uk
RCEM/TOXBASE SNAP Protocol — toxbase.org
GEMNet Guideline for TCA Overdose Management — Emerg Med J 2011
NPIS (National Poisons Information Service) — npis.org